My Village My Home: A Tool to Strengthen Community Involvement in Immunization
Health practitioners are constantly looking for tools that reliably advance knowledge or bring about much needed change. When opportunities to share proven tools in new locations or different communities arise, they are eager to seize the chance at using a solution that can solve their communities’ health challenges. Such is the case of My Village My Home (MVMH), a simple tracking tool that facilitates community engagement and mutual accountability to promote immunization.
The MVMH tool is made up of a 100 cm long visual dashboard whereby every infant in a community has his or her own row on the tracker, with spaces for the child’s name, date of birth, and dates of each vaccination clearly marked. A roof covers the listings to show that the community is like a house whose strength depends on the quality of the supporting materials – in this case bricks or blocks, each of which represents one vaccination dose for each child. When each brick in the child’s row is complete, the child is fully immunized, which contributes to protecting the whole village from Vaccine Preventable Diseases (VPDs). Empty bricks represent missed vaccinations, rendering the community vulnerable. The MVMH tool was designed to be large enough that when hung in a community setting, or shared meeting space, the vaccination status of all the children in the community is clear.
At A Glance
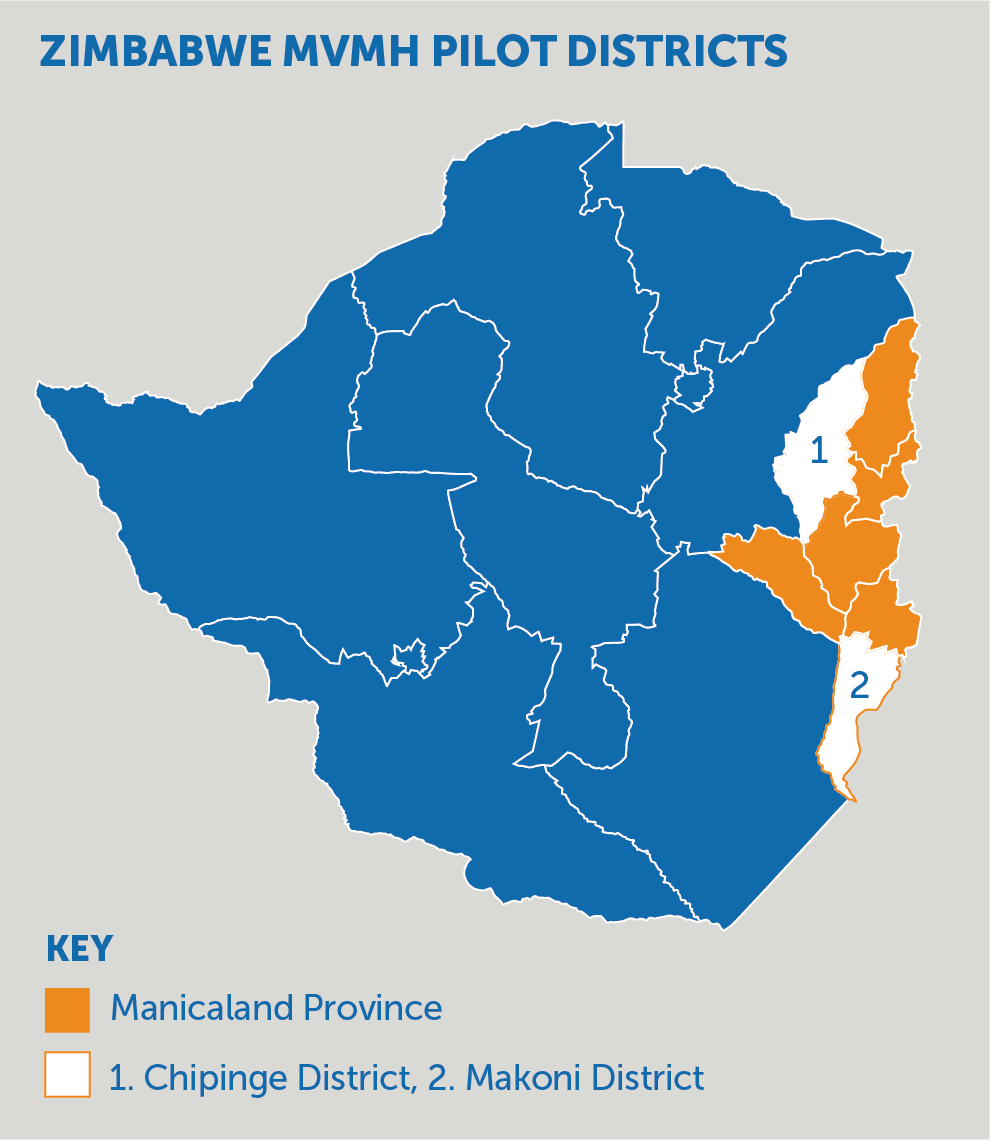
An Immunization Technical Officer with JSI, Coscar Zvamashakwe, is one of the change champions who has been instrumental in using the MVMH tool in her home country of Zimbabwe. In 2017 a situational analysis was conducted in Manicaland Province in eastern Zimbabwe under the Maternal and Child Health Integrated Program (MCHIP), funded by USAID with technical support from John Snow, Inc. ( JSI). Findings indicated that one of the drivers of low coverage was inconsistent vaccination visits by caregivers. In addition, despite a high number of facility births, many children were never captured in the EPI registers due to weak tracking mechanisms. As such, it was difficult to know which child was due for which vaccine and by when. Coscar learnt about the MVMH tool with interest while attending a regional meeting on the Reaching Every District/Reaching Every Child approach, which was also attended by JSI colleagues from Malawi who were implementing the MVMH approach in their country. The cultural influences around responsibility and shared accountability resonated with Coscar and she felt that the MVMH tool held potential to address some of the immunization coverage and equity challenges in Manicaland. With funding from the Bill & Melinda Gates Foundation, an 8-month pilot was designed to take place in 2017 in Chipinge and Makoni Districts.

Source: JSI
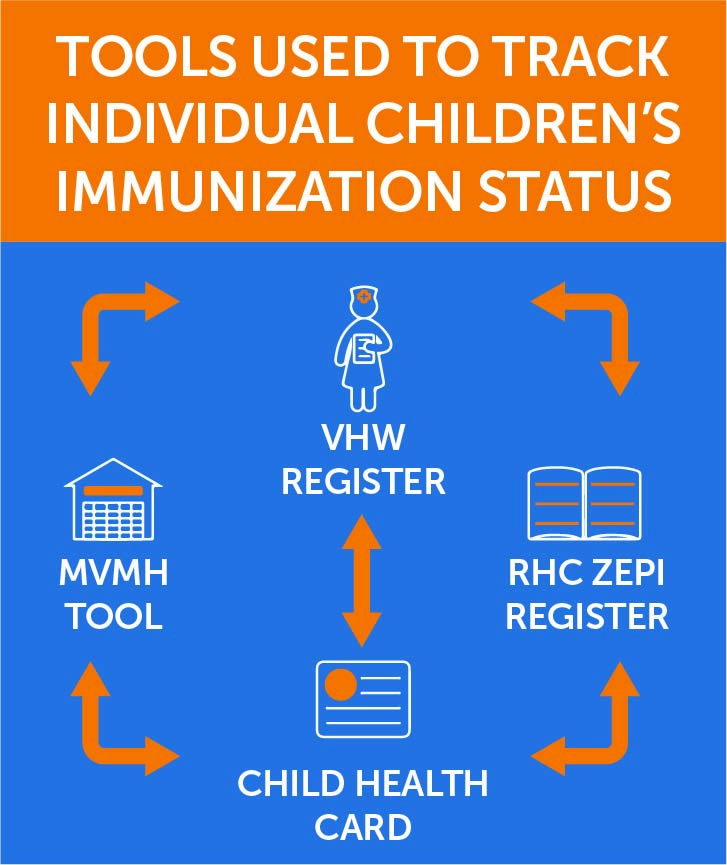
Coscar identified and trained Village Heads and village level health workers (VHWs) to use the MVMH tool in their villages, which had anywhere between 20 and 200 vaccine-eligible children. Together with the EPI and her team, Coscar trained the VHWs to collect and manage the data with the expectation that they would be the new custodians of the information that would in essence ‘hold the village up’. VHWs first conducted home visits and recorded the names of all the children below the age of two in their catchment area. During these visits, they would examine the Child Health Cards (CHCs) presented by the caregivers and record the immunization information into a VHW register. At the close of each month, the VHWs would compare their register with the local health facility’s Zimbabwe Expanded Programme on Immunisation (ZEPI) register. Once aligned, the information was transferred onto the MVMH tool, which was kept by the Village Head, for follow-up in the village. The overall objective of the VHWs work was to ensure matching data across the CHC, the VHW register, the facility ZEPI register and the MVMH tool, and then work with the health facility and village heads to ensure children received their vaccinations on time.
At first, the process of filling out eligible-children names and recording the vaccinations in the MVMH tool took a long time – especially for the villages with high numbers of children below 2 years. But as time went on and familiarity with the process grew, maintaining the record became seamless. Soon the VHWs were only adding one to three names of infants each month as they were born.
The pilot revealed the tool’s effectiveness in involving Village Heads and VHWs as agents to have a more complete listing of infants in their catchment areas and identify and reach children who had missed vaccinations. Village Heads could easily track children who had missed vaccinations and work with the VHWs to follow up and ensure the children received their vaccines. Both parties showed remarkable consistency in hosting community meetings using the MVMH tool as a discussion point to showcase the importance of timely and complete vaccination. With the openly accessible and communally discussed tool, there was increased community awareness on immunization as essential for the protection of their children.
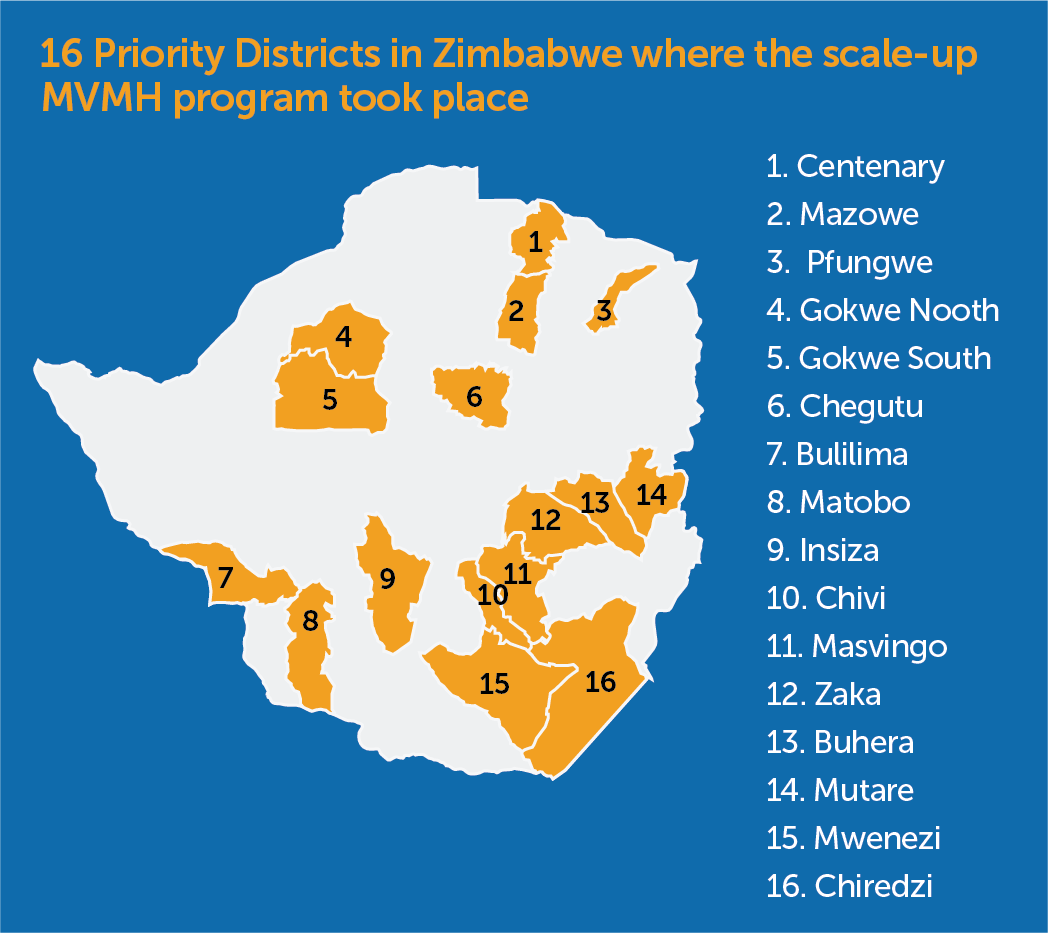
Impressed with the community participation approach in building shared responsibility for the health of children, the Ministry of Health and Child Care (MOHCC) approved roll out to 16 additional priority districts with similar low routine immunization coverage and scale-up began at the start of 2018 with funding support from Gavi, the Vaccine Alliance.
Zimbabwe now sits on the list of countries with consistent improvement in routine immunization and remains a relevant example of how a shared resource can go beyond its original scope to bring about change both near and far.

Adelaide Shearley
This Bright Spot Story was nominated by the late Adelaide Shearley (seated in the middle), a Regional Immunization Technical Adviser with JSI in Zimbabwe. Adelaide was keen to share this story to highlight the importance of sharing learnings amongst different areas, communities, and countries, especially in an era of dwindling resources for immunization. It was Adelaide along with Coscar who first learned about the MVMH tool from her JSI colleagues in Malawi and saw the potential for its success in Zimbabwe. This Bright Spot is dedicated to Adelaide, who sadly passed away in January 2021, one of millions of casualties worldwide of COVID-19. Her dedication, energy, and passion were the driving force behind our successful partnership and success in Zimbabwe, and in the communities she served.