Multiple Battles: Vaccinating Zero-Dose Children in Conflict Zones in Niger
In May 2022, Sabin’s Boost Community and the World Health Organization (WHO) launched the first cohort of the "COVID-19 Recovery for Routine Immunization Programs Fellowship". The aim of this program was to strengthen the capacity of national and sub-national immunization professionals to plan and implement immunization programming during the COVID-19 recovery period, with the ultimate goal of reversing the declining rates of immunization coverage. After an intensive live engagement series, Fellows were tasked with drafting their own strategic proposal for implementation or case study for publication. This series of Bright Spots share Fellows' key learnings and takeaways from the program.
Charles Keamou Thea, a physician and epidemiologist in Niger and Head of the World Health Organization (WHO) Sub-Office in the Tahoua region, was seeking an opportunity to reduce the number of zero-dose children in Tahoua, especially those from displaced families, when he received an email shared through the WHO Niger mailing list about the 2022 COVID-19 Recovery for Routine Immunization Programs Fellowship. The Fellowship, offered by the Sabin Vaccine Institute’s Boost Community and World Health Organization (WHO), provided an opportunity to strengthen the capacity of immunization professionals, like Charles, to recover and bolster immunization programs in their countries.
The Tahoua region recorded its first case of COVID-19 in April 2020, shutting down many of the health services in the area. By June 2020, over 7,200 children were recorded as “zero-dose,” or not having received any life saving vaccinations. By August 2021, that number reached more than 11,700, compared to pre-pandemic numbers (from 2019), which were between 1,500 and 2,000 zero-dose children in the region. Parts of Tahoua border the Republic of Mali, where non-state armed groups have committed armed attacks and kidnappings in both Mali and Tahoua, forcing many people to escape to central and southern districts of the Tahoua region. Several of the identified zero-dose children were from these displaced families.
Number of Zero-Dose Children in Tahoua Region, Niger
Engaging Key Stakeholders to Improve Vaccine Coverage
Charles’ Fellowship project focused on vaccinating zero-dose and insufficiently vaccinated children in security-compromised zones in Tahoua Department, Keita, and Bouza, all located within the Tahoua region of Niger.
Charles began the project with an analysis of immunization data by his team at the Tahoua WHO sub-office and the regional office immunization team. Next, the teams mapped zero-dose children in the areas with low vaccination coverage. After that, Charles and his colleagues hosted an advocacy meeting, which brought together opinion leaders, administrative authorities, mayors, religious leaders, and defense and security forces. Charles presented on the state of vaccination in security areas as well as on the impact of COVID-19 on health services. District medical officers, immunization officers, and heads of health centers proposed solutions for catch-up vaccination of zero-dose children. Upon the close of the meeting, Charles received the commitment of attendees to be involved in his project.

Vaccination Campaigns in the Midst of Conflict
Charles hosted coordination meetings with his team and the district management team in order to plan advanced and mobile vaccination activities in the villages and nomadic corridors as well as during transhumant, or the seasonal movement of breeders or farmers from one place to another with a well-marked and known itinerary. Engagement with community members allowed the team to obtain information on new households and map the community as well as determine areas to run mobile vaccination sites. Mobile vaccination sites were then set up at sites for Internally Displaced Persons as well as at pastoral wells and in corridors. Awareness raising was carried out through community relays, where Charles’ team searched for unvaccinated children and educated their parents on health services and vaccination. Within each area, the team worked with healthcare professionals involved with vaccination, such as chief physicians, immunization officers, and health center chiefs.

Charles and his team collectively pooled resources with the health districts to resolve logistical difficulties, such as the moving of households from one location to another which required further resources, staff, and transportation to accommodate. Charles lauded the aid of the funding provided by the Fellowship as well as his Fellowship mentor who “always responded to emails and provided input on time.” In particular, Charles said, “my mentor guided me through the development of the project, the analysis and interpretation of the results and the writing of the final report.”
However, challenges arose with the increasing number of internally displaced people fleeing their home regions and entering Tahoua, resulting in many new people to vaccinate. Additionally, there was especially low vaccination coverage among this population, leading to an increase in cases of measles and diphtheria in the area.

Despite these obstacles, Charles said “the involvement of opinion leaders and the participatory approach were innovations” in his region and contributed to the success of his project. The team engaged opinion leaders and identified focal points within the displaced populations as part of their awareness-raising activities. He highlighted the importance of involving all community actors (administration, military, civil society, traditional and religious leaders) in project planning and implementation, especially by using a community-based, participatory approach.
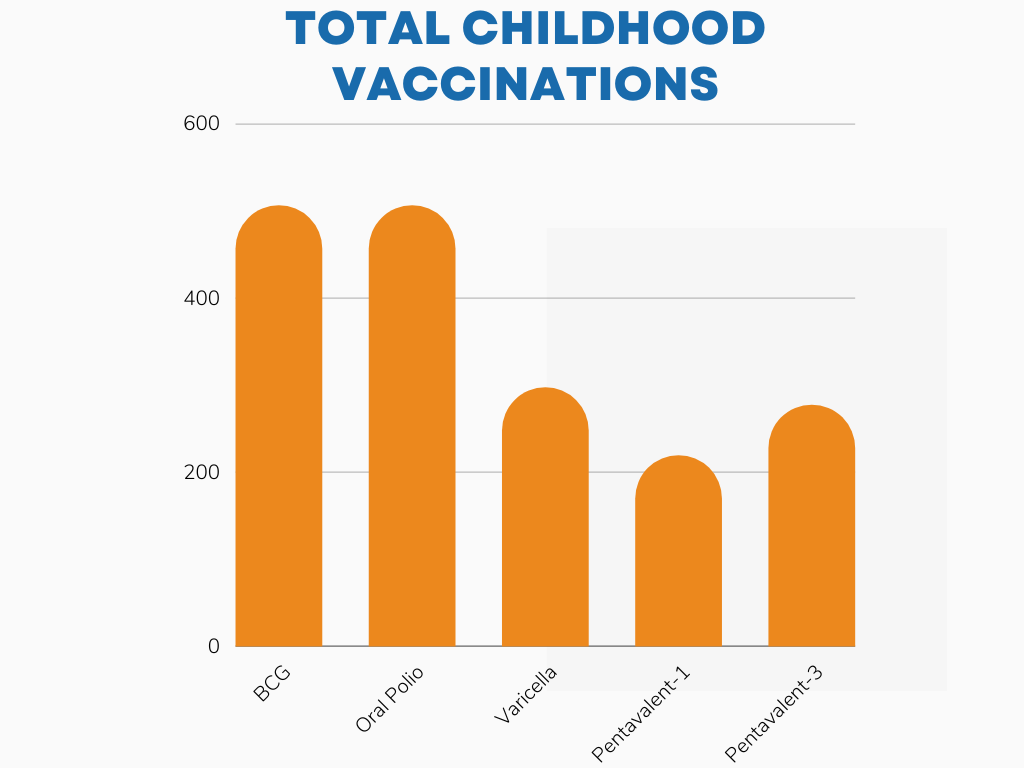
The project began in November 2022 and concluded in February 2023. During this time period, Charles and his team succeeded in vaccinating 506 children with the Bacille Calmette-Guerin (BCG) and oral polio vaccines; 297 children with the varicella (VAR-1,VAA) vaccines; 219 children with the first dose of the pentavalent vaccine; and 277 children with the third dose of the pentavalent vaccine.
Final Results
Although the project has been completed, Charles ensures there is continual monitoring and evaluation of vaccine coverage by age group in these localities in place. Charles hopes to strengthen and expand his project into other localities with compromised security and among special populations, such as internally and externally displaced people and nomads.

2022 Fellow & Contributor
Charles is a public health physician, specializing in epidemiology and community health. He serves as an international consultant for the CDC/ATLANTA STOP POLIO 53 program. He has worked in immunization for over 10 years and most recently served as Head of the WHO Sub-Office in the Tahoua region, working with the STOP Polio Eradication Program and coordinating all of the country office’s health programs.
