Reducing Zero-Dose Children in Gbarpolu County, Liberia
In May 2022, Sabin’s Boost Community and the World Health Organization (WHO) launched the first cohort of the "COVID-19 Recovery for Routine Immunization Programs Fellowship". The aim of this program was to strengthen the capacity of national and sub-national immunization professionals to plan and implement immunization programming during the COVID-19 recovery period, with the ultimate goal of reversing the declining rates of immunization coverage. After an intensive live engagement series, Fellows were tasked with drafting their own strategic proposal for implementation or case study for publication. This series of Bright Spots that shares Fellows' key learnings and takeaways from the program.
Introduction
Gbarpolu County, one of the largest counties in Liberia, has faced ongoing challenges with increasing routine immunization rates. The county was created in 2001 and is not only Liberia’s youngest county but also one of the most inaccessible and under-developed. Gbarpolu County’s lack of health infrastructure – there are only fifteen clinics and a single hospital serving approximately 450 diverse communities – leaves much of the population without easily accessible health services. According to a 2021 equity assessment, approximately 68% of the population in Gbarpolu, particularly those in remote areas, must walk more than 60 minutes or five kilometers to reach the nearest facility. Many parents and caregivers must therefore travel long distances on foot over bad roads and/or pay substantial transportation costs to access immunization services, often becoming demotivated to return for subsequent doses. Furthermore, Gbarpolu County is known for its highly migratory population that moves between communities based on mining conditions. This transient population causes challenges for planning immunization services and meeting coverage targets.
With this poor access to health facilities, low routine immunization coverage rates and high drop-out rates were exacerbated by the disruption of services due to the COVID-19 pandemic. The Penta1 and MCV1 coverage in Gbarpolu County dropped by 2.6% and 5.4%, respectively, from 2019 to 2021. Further analysis of immunization performance in the county has shown that the number of zero-dose (ZD) children, those who have not received any life-saving vaccines – specifically, their first dose of Penta1 – has also increased by 14% over the last three years from 939 in 2019 to 1,073 in 2021. Reversing these poor trends in coverage, drop-out rate, and number of zero-dose children in one of the most challenging terrains was prioritized for this project.
| Table 1. Showing Coverage of Pentavalent-1 and MCV 1 of Gbarpolu County and Liberia, 2019-2021 | ||||
|---|---|---|---|---|
| Year | Antigen | Gbarpolu's Coverage | Country's Coverage | |
| - | 2019 | Penta1 | 78% | 94% |
| - | 2019 | MCV1 | 70% | 85% |
| - | 2020 | Penta1 | 76% | 90% |
| - | 2020 | MCV1 | 63% | 82% |
| - | 2021 | Penta1 | 75.4% | 89% |
| - | 2021 | MCV1 | 64.6% | 75% |
Intervention
Matirankie Kanneh designed a community-centric process to increase immunization coverage, with a focus on strengthening community participation and ownership of the planning, decision-making and implementation of immunization services. Co-funded by the COVID-19 Recovery for Routine Immunization Programs Fellowship and UNICEF, the Ministry of Health (MoH) and County Health Team implemented a six-step process from September 2022 through January 2023 to reduce dropout rate for Penta 1/Penta 3 by 5% (from 12% to 7%) and for Penta 1/MCV1 by 7% (from 14% to 7%). Their strategy included expanding the network of service providers (vaccinators, Community Health Volunteers, and Community Health Assistants) and peer ambassadors, and increasing access to immunization services through intensified outreach services.
1. Inception meetings with county, district, and health facility staff
- A series of inception meetings laid the foundation for project activities and ensured support from key stakeholders.
- A project inception meeting brought together county health authorities, partners, and national EPI supervisors via Zoom to discuss the project objective, activities, deliverables, expected outcomes, as well as the roles and responsibilities of all involved.
- Through an in-person county inception meeting, county-level health stakeholders, district-level supervisors, and in-county partners met to review objectives and expectations and provide space to discuss concerns and challenges. Key discussion points included support for health facilities without functional cold chain equipment and how to provide supplemental cold chain devices and fast cold chain services.
- In health facility meetings, participants – including vaccinators, Officers In-Charge, Certified Midwives, Registrars, and Community Health Services Supervisors – developed a chronogram of activities and an implementation tracker using MS Excel for weekly/bi-weekly reporting. Following these meetings, county, district, and health facility authorities, as well as staff, showed excitement and readiness to take the lead in planning and implementing the activities.
2. Advocacy meetings at county and district levels
- Stakeholder advocacy meetings, at the county and district levels, aimed to strengthen community ownership and participation in immunization planning and decision-making, as well as provide a platform to identify advocates to champion immunization messaging. Meetings were led by County or District Health Officers, with support from supervisors from EPI and the MoH, and brought together a wide range of participants, including influencers, traditional leaders, civil society organizations, actors, and religious leaders. Additional participants included representatives from the Agricultural Ministry, Gender Ministry, Ministry of Education, Liberia Marketing Association, Gbarpolu Network of Churches, and National Imam Council in Gbarpolu were also present. The meetings served to strengthen stakeholder buy-in and receive feedback and support on the project.
Key messaging was developed in these meetings to be shared with communities, such as:
- “All children born across the country are to visit hospitals/ clinics/vaccination sites six times before the age of two years old.”
- “Girls nine years of age are to receive HPV vaccines.”
- “Vaccines are safe, free, and available.”
- “County Education Officer and county level Imam heads and Pastoral boards should serve as immunization ambassadors.”
3. Microplanning sessions at health facilities and district levels
- Micro-planning was used to ensure that immunization services reach every community and all targeted beneficiaries. District supervisors led the micro-planning process, working with health facility and community-level health workers to identify priority communities and plan actionable solutions that peer ambassadors could immediately implement. Communities prioritized for this project included those that are underserved, difficult to reach, face barriers to access and utilize immunization services, and special populations, among others.
- Vaccinators at the health facility reviewed their immunization ledgers to identify mothers who were frequently and timely bringing their children for vaccination. When identified and located, they were engaged to serve as peer ambassadors and vaccine champions for their communities and anywhere else they could use their story to convince other people to get their children vaccinated.
- The micro-planning process also identified community-level influencers and forecasted vaccine supply needs. A new and improved paper-based template was used for this process at the health facility levels; the data was input, interpreted, and summarized at district levels using Excel.
4. Recruitment and assignment of 90 peer to peer immunization ambassadors in prioritized communities
- The peer ambassadors played a crucial role in building sustained immunization networks among community members. They served as vaccine champions, seeking to convince mothers to take their children to the health facility for vaccination, receiving an honorarium for their efforts. They worked to raise awareness about immunization, identify children who were unvaccinated or had missed doses, provide reminders for immunization appointments, and encourage others to consistently utilize immunization services and attend outreach sessions. To effectively engage with their communities, peer ambassadors utilized different women-based group platforms and gatherings, such as local creek/riverside washing, to interact with one another.
- Supervisors provided on-site mentoring and conveyed the expected outputs to the peer ambassadors. During this process, supervisors emphasized the importance of commitment and assessed the ambassadors’ ability to carry out these activities. Peer ambassadors who consented to serve were encouraged to continue this work even beyond the project, becoming recognized as Immunization Ambassadors in their respective communities. As national immunization campaigns continue to be conducted, peer ambassadors are key in improving immunization coverage.

5. Special outreach teams recruited and assigned to hard-to-reach areas
- In addition to the monthly outreach provided by health facility staff, special outreach teams consisting of trained health workers were recruited and assigned to identify communities and market areas to provide intensive outreach services. During the micro-planning process, catchment communities with high numbers of unimmunized or under-immunized individuals or those located in remote or geographically challenging terrains were identified and targeted for these outreach services.
- Two strategies were used. The first included health facility-based outreach, which was planned and carried out by health facility service providers twice a month in communities between 5-10 kilometers or 1-2 hours walking distance from the facility. The second strategy focused on supervisors recruiting outreach teams at the district and county level. Once teams were created, outreach services were held over a five day period every month. Teams were tasked to reach and provide services to remote areas, defined as more than 10 kilometers from the nearest health facility, and to the hard-to-reach mining communities. Market areas were also used to provide services by the outreach teams.
- The teams recruited and permanently assigned 30 Community Health Assistants/Volunteers (CHA/CHV) to their communities. These CHAs/CHVs were selected by the community itself and were residents of the assigned communities. Their responsibilities included conducting door-to-door awareness campaigns, identifying unvaccinated or under-vaccinated individuals, maintaining a registry of immunization status, and referring individuals to the appropriate health facilities. The CHA/CHVs gained more knowledge and experience on how to identify immunization defaulters, missed children, and ZD children and what strategies work to routinely keep up with immunization coverage.

6. Supportive Supervision and Monitoring Across District, County and National-Level
- The project implementation and monitoring process involved the use of an approved checklist. This checklist was utilized by three different levels of supervision: district, county, and national. Supervisors conducted visits to various implementation sites and provided mentoring to field implementers and vaccination teams, which included special outreach staff and supervisors, ensuring they were aware of their targets and familiar with the different strategies being employed in the project.
- Supervisors also verified the accuracy of outreach schedules and assessed the implementation status of activities. They closely monitored the utilization of logistics and other forms of support provided to the implementers. Additionally, supervisors actively sought feedback from the implementers, encouraging them to share any challenges or recommendations for project improvement.
- The project activities were implemented according to the original proposed timeline; however, certain adjustments were made. One such adjustment involved modifying the number of peer-to-peer ambassadors to ensure effective monitoring and accommodate budget changes. It was proposed to increase the number of community peer ambassadors from 90 to 150 due to the significance of the peer ambassadors’ efforts. The team was able to accomplish this by incorporating the 60 peers who were initially supported by UNICEF, expanding reach to 150 communities.
Results
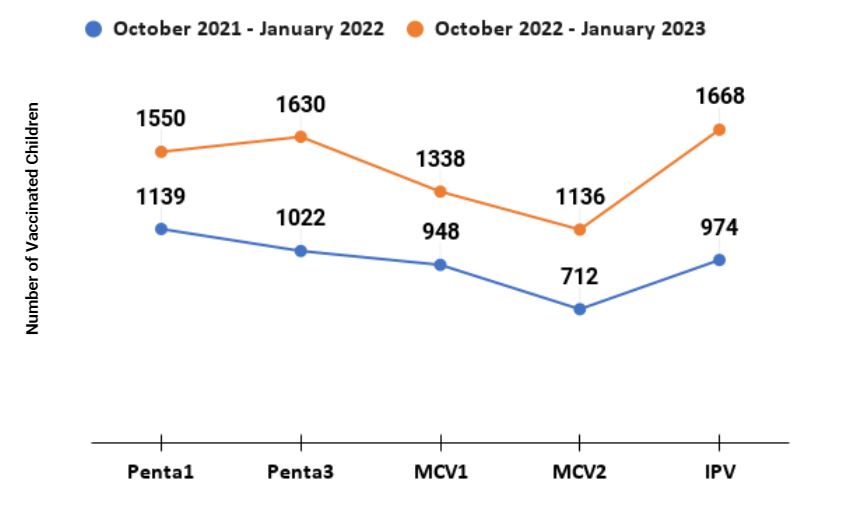
As detailed in Table 2, 2650 children under the age of two were vaccinated with Penta1, Penta 3, MCV1, and MCV2 during outreach sessions conducted by the vaccinators in their usual catchments within a period of four months (October 2022 – January 2023). HPV1 was administered to 770 nine year-old girls in the same period during the outreach sessions, with a second dose given to 527 girls.
Figure 1 illustrates the year-over-year comparative analysis of the number of children under two years-old immunized in Gbarpolu County (October 2021-January 2022 vs October 2022-January 2023. Significant increases in the number of children vaccinated were achieved, including a 36% increase in Penta1 doses, 60% increase in Penta3, 41% increase in MCV1, 60% increase in MCV2, and a 71% increase in IPV. Similarly, the number of fully immunized children at age 2 increased from 708 to 1094, a 55% increase.
| Table 2. Vaccine Doses Given During Outreach Sessions, Gbarpolu County | ||||||
|---|---|---|---|---|---|---|
| Penta1 | Penta3 | MCV1 | MCV2 | HPV1 | HPV2 | |
| Oct-22 | 255 | 255 | 146 | 143 | 249 | 156 |
| Nov-22 | 160 | 182 | 183 | 121 | 165 | 146 |
| Dec-22 | 142 | 216 | 131 | 124 | 178 | 100 |
| Jan-23 | 147 | 178 | 136 | 131 | 178 | 125 |
| Total | 704 | 831 | 596 | 519 | 770 | 527 |
Figure 1. Cumulative Number of Children <2 years Immunized Before and After Project, Gbarpolu County
Lessons Learned
During project implementation, strong and effective collaboration with local stakeholders in the planning and implementation of projects promoted ownership and was key to obtaining success and sustaining gains. High-impact results can be achievable with limited resources if there are clearly defined strategies and a willing and motivated team.
Proper micro-planning was key in identifying zero-dose children and missed communities and prioritizing where efforts should go. This targeted, data-based approach proved instrumental in maximizing the impact of interventions and ensuring success in reaching the most vulnerable populations. The paper-based template developed for this project added value for the County Health teams, who hope to continue with them in the future.
Looking Forward
The project team recommends that the MoH and partners should conduct comprehensive capacity building for supervisors and vaccinators at all levels. Steps should be taken to also strengthen the integration of COVID-19 vaccination opportunities to provide routine immunization services and vice versa. Finally, to sustain the progress made, key project activities should be incorporated into the community health toolkit’s subsequent plans.
For the future, the project team suggests conducting two more rounds of this initiative in 2023 to consolidate gains and reduce defaulters and zero-dose children. Teams should continue to work with the County Health teams and the Ministry of Health to use evidence-based data to identify and solicit support for counties that are lagging in immunization coverage.
References
- Hussein, Gradiah Walker Bou. “Hope on the Horizon: Improving Immunization Access in Hard-to-Reach Areas of Liberia.” UN Liberia |UN, 16 June 2023, https://liberia.un.org/en/236789-hope-horizon-improving-immunization-access-hard-reach-areas-liberia

2022 Fellow / Contributor
This study is shared by Matirankie M. Kanneh. Ms. Kanneh is a Liberian female who has worked with the health system at health facility, county, and national levels for more than 10 years. In 2022, she worked for the Ministry of Health at the national level as the Routine Immunization Coordinator. She is currently a candidate for a Master’s of Public Health in Epidemiology and works at Frontier Health Markets (FHM) - Engage, a USAID funded global cooperative as an Immunization Specialist.
