Disparity in Access to Routine Immunization Services Among Children Under 5-Years Old in Myanmar
In May 2022, Sabin’s Boost Community and the World Health Organization (WHO) launched the first cohort of the "COVID-19 Recovery for Routine Immunization Programs Fellowship". The aim of this program was to strengthen the capacity of national and sub-national immunization professionals to plan and implement immunization programming during the COVID-19 recovery period, with the ultimate goal of reversing the declining rates of immunization coverage. After an intensive live engagement series, Fellows were tasked with drafting their own strategic proposal for implementation or case study for publication. This series of Bright Spots that shares Fellows' key learnings and takeaways from the program.
Introduction
Myanmar has been severely affected by the COVID-19 pandemic and ongoing political crisis, resulting in a fragmented health system and difficulties in accessing essential health services , including routine immunization. The ongoing political crises have disrupted health services due to insecurity of healthcare personnel and damage to health infrastructure. Moreover, Myanmar’s wide geographic disparity and hard-to-reach regions, sociocultural diversity with more than 135 ethnic groups, societal insecurity, and increased population mobilization due to sporadic conflict between various armed ethnic groups has caused challenges in healthcare delivery.
As a consequence, accessing vaccination services has been incredibly difficult for much of the population and routine immunization rates in Myanmar experienced a significant decline. Myanmar had succeeded in achieving high immunization rates by 2019, with BCG coverage at 92% among children under the age of five, and OPV-3 & Penta-3 coverage at 91%. However, in 2021, these rates dropped significantly, to 48% BCG coverage, 43% OPV-3 coverage, and 37% Penta-3 coverage. Assessing the disparity in access to routine immunization services and the factors that influence on access to routine immunization service utilization across the different geographic areas of Myanmar, including cultural norms and beliefs, will provide baseline information to design responsive immunization delivery plans to improve access to routine immunization service delivery in Myanmar and increase readiness to respond to vaccine-preventable disease outbreaks in the future.
Intervention
A mixed-methodology population-based study was undertaken to explore how three townships in Myanmar utilized routine immunization services during the COVID-19 pandemic and explore what factors influence the communities to access routine immunization services. In order to identify communities that are representative of Myanmar’s geographic diversity, the 14 administrative areas that comprise Myanmar were divided into three clusters based on common characteristics (hilly, coastal, and central plateau), and one township was randomly selected from each cluster.
This study included a cross-sectional quantitative interview of mothers and caregivers of children under five years-old and in-depth qualitative interviews with local stakeholders, including mothers and caregivers, religious and community leaders, and healthcare providers. The finite population proportion formula was used for the cross-sectional study, with a total sample size of 417.
The WHO Behavior and Social Drivers (BeSD) framework was used to guide for questionnaire development, enabling the study team to explore the underlying factors influencing vaccination decision-making in Myanmar. The BeSD framework explores the beliefs and experiences specific to vaccination that could be modified to increase vaccine uptake, focusing on four key domains: thinking and feeling, social processes, motivation, and practical issues. For this project, the BeSD was initially developed in English and translated into Burmese. To ensure the efficacy of the methodology and reliability of the questionnaire, a pilot test was conducted in a nearby township.
Three research assistants were trained to carry out both quantitative and qualitative data collection, including interviews. Though face-to-face interviews were planned, phone interviews were ultimately conducted due to active conflict in some of the selected study areas and restrictions by local authorities.
Results
From November through December 2022, quantitative cross-sectional surveys were completed by 102 participants in the selected hilly cluster township and ten qualitative interviews were conducted with community representatives, including three mothers, two caregivers, one religious leader, one teacher, one community leader, one healthcare provider, and one representative of a philanthropic organization. Data collection occurred in the selected coastal cluster and central plateau townships from February through the second week of March, collecting an additional 315 quantitative surveys (223 in the coastal cluster township and 92 in the central plateau township) and ten qualitative interviews per township. In total, 417 participants completed the cross-sectional quantitative questionnaire across all three study areas, yielding a respondent rate of 100% in each area.
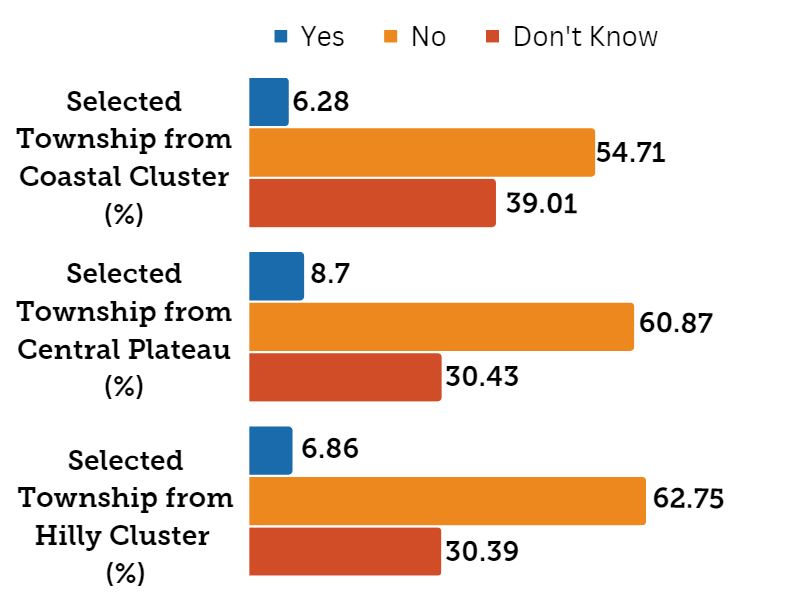
Among the participants, across the three study areas, an average of 59.44% respondents reported their children have not received the scheduled vaccines within the past year. Only an average of 7.28% reported their children received vaccination within the past year. An average of 33.48% of respondents reported they did not know whether their child received all scheduled vaccines. To view township breakdowns, refer to Figure 1.
Figure 1: Knowledge of Children's Vaccination Status in Three Study Areas
Utilizing a Chi-squared test (Table 2), the analysis reveals that the factors linked to vaccination status among children under five years-old vary by township. For instance, in the selected township from the coastal cluster, factors associated with vaccination status within the last year (p-Value <0.05) included gender, ethnicity, education, occupation, age of youngest child, respondent type, family member role, emotional perceptions, willingness of community leaders, health worker’s recommendation for vaccination, motivation, and practical issues. In the selected township from central plateau, factors associated with vaccination status within the last year (p-Value <0.05) included ethnicity, vaccine stockouts, receiving information about routine vaccinations, and overall satisfaction with vaccination services. In the selected township from the hilly cluster, factors correlated with vaccination status within the last year (p-Value <0.05) included willingness, receiving reminders, awareness of vaccination locations, receiving information related to vaccination information, accessibility of vaccination services, and satisfaction with the vaccination services.
30 in-depth qualitative interviews across the three study areas contributed additional insight into community members’ thoughts and feelings regarding childhood vaccination programs, vaccine availability, and the information that has influenced their decision-making. For example, mothers and caregivers reported concerns about vaccine side effects, inability to access vaccination services, either due to vaccination dates/times that conflicted with their work schedules or lack of transportation challenges, and lack of knowledge. Others reported challenges including safety concerns at vaccination sites and misinformation circulating on social media.
To see further socio-demographic characteristics, visit the Annex, Table 1.
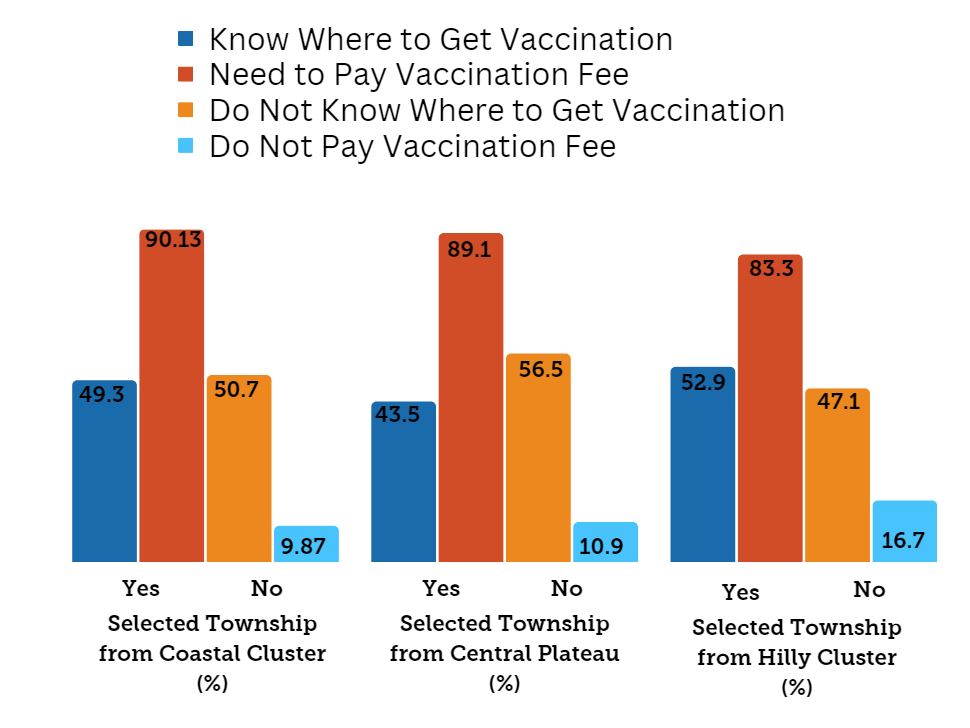
Quantitative survey results support the insights shared through qualitative interviews. Only 16.40% of respondents across the study areas wanted their children to receive all scheduled vaccines and 58.94% preferred their children to not receive any of the scheduled vaccines; study area specific results are included in Figure 2. Access and practicality issues are also evident, as seen in Figure 3 – more than 88% of all respondents were required to pay vaccination fees through donation boxes and more than half of respondents did not know where to get vaccinations
Figure 2: Percent of Respondents Who Say They Want Their Child to Get the Scheduled Vaccines
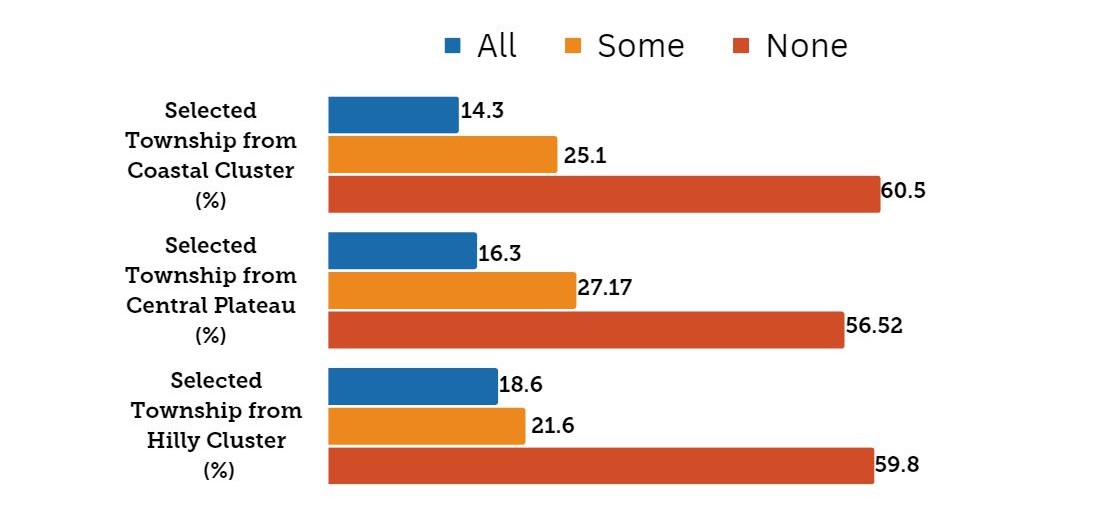
Figure 3: Practical Issues Among 3 Study Areas
Lessons Learned
This study revealed considerable insights regarding factors that influence access to routine immunization service in Myanmar that can be used to design immunization delivery plans that respond to local context and needs. However, it is important to note the substantial lack of knowledge on behalf of mothers and caregivers regarding the vaccines their children had received. Over one-third of participants were unaware if their children had received vaccines according to the recommended schedule, and almost all participants reported having not received their child’s vaccination card. To enhance knowledge of vaccination programs and schedules for upcoming vaccines, providers should consider giving vaccination cards directly to mothers or caregivers, thus involving mothers and caregivers in the vaccination process and increasing their knowledge and awareness.
Furthermore, even among the mothers and caregivers that were aware of their child’s vaccination status, the study population impacted results. The study questionnaire asked about vaccination status within the last year, however the study population included mothers and caregivers of children under five years old. The children who were three or four years old who had received all routine immunizations according to schedule would still have not received any vaccines within the last year – thereby likely impacting results. Modifying the study population to mothers and caregivers under two years old would be more appropriate and likely provide higher quality data.
Additionally, childhood vaccination rates could potentially be elevated by employing the Information, Education, and Communication (IEC) approach through digital technology, community awareness sessions, and women’s empowerment. Vaccination programs concentrating on childhood immunization could also adopt a parent-centered/availability approach. The involvement of community-based organizations for transportation and encouragement would aid in ensuring eligible children receive their vaccinations. Additionally, translating vaccine information into major ethnic languages would promote equitable access to information.
Finally, the political and cultural context in Myanmar had significant impacts on both the methodology of this study and results seen. For example, the WHO BeSD framework used for the development of the quantitative cross-sectional questionnaire included factors that were not applicable in the local context. Within the Myanmar health system, all provider recommendations must be followed – therefore factors such as “respect from health workers” and “vaccine confidence” were not applicable. Similarly, conducting the study during a period of political turmoil with prevalent security concerns impacted the ability of the study team to collect data in-person, while online surveys were not feasible due to limited internet connection. In order to successfully collect data from diverse perspectives, the study team reached participants through phone calls instead.
Looking Forward
The insights from this study will be used to advocate for policy improvements, engage interested partners, and collaborate with multiple stakeholders to enhance vaccination status among children under five years old in Myanmar. Collaboration with stakeholders and partners will also be pursued to strengthen demand (via immunization awareness campaigns), develop digital reminders to reduce missed appointments, and create e-vaccine certificates.
This study will further be enhanced by modifying the study population to mothers and caregivers of children under two years old, and then expanding data collection to the remaining 11 administrative areas of Myanmar.
References
- “The Republic of the Union of Myanmar: Ministry of Labour, Immigration and Population – Department of Population.” Pritzker Legal Research Center | Northwestern, https://library.law.northwestern.edu/myanmar/population
- “The Civil War in Myanmar 2023 Conflict Diagnostic.” Carleton University | reliefweb, 6 March 2023, https://reliefweb.int/report/myanmar/civil-war-myanmar-2023-conflict-diagnostic
- “Increasing vaccination demand and uptake.” Essential Programme on Immunization | World Health Organization, 2022, https://www.who.int/teams/immunization-vaccines-and-biologicals/essential-programme-on-immunization/demand
Annex (see PDF)
2022 Fellow / Contributor
This case study was shared by Dr. Nway Ein Chei who holds positions such as Ambassador of the Myanmar of ESG Society Organization and Advisor of HOPE NFT Organization in Hong Kong. She is also a Visiting Lecturer at Myanmar Creative University. Dr. Chei earned her Bachelor’s in Medicine and Surgery at the University of Medicine Magway, a Master’s in Public Health and is currently a Doctoral candidate for the Public Health Program (Global Health) at Mahidol University. With over eight years experience, she held roles like Research Medical Doctor, General Practitioner, Volunteer Telemedicine Consultant, Zonal Health Specialist, Health Technical Program Coordinator and Immunization Officer for Primary Health Care, Nutrition, Maternal and Child Health at various organizations. She has won the Second Runner-Up in the Business Plan Competition of the United Nations South-South Entrepreneurship Academy and selected as a Young Professional candidate for the global health education program at Health and Global Policy Institute, Japan. She received National Volunteer Steering Unit’s Honor of Certification for Volunteerism in Myanmar COVID-19 response and has been offered as Country Representative of the Harpswell ASEAN Young Women Leadership Program. Dr. Chei has published three articles in the book “Metaverse Mindset (Virtual and Real) Transformations with Impacts via SDGs”. Her comprehensive achievements highlight her dedication to global health.
